

What Is a Lipoma?
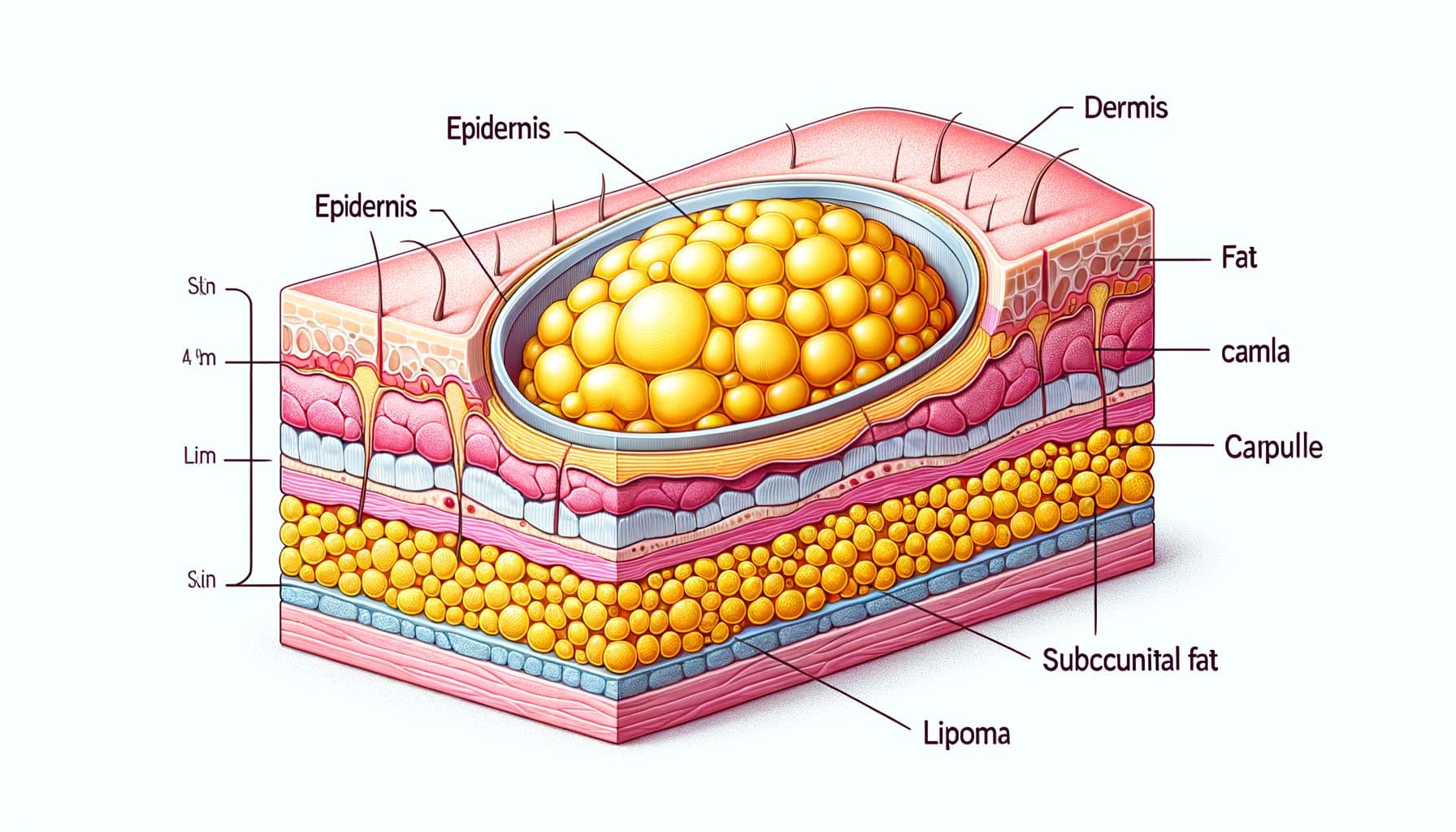
A lipoma is a benign (non-cancerous) tumor composed of mature adipose (fat) cells that develops in the subcutaneous tissue — the layer of fat between the skin and the underlying muscle. Lipomas are the most common soft tissue tumors in adults, with an estimated prevalence of approximately one percent of the general population, though the true figure is likely higher as many small lipomas go unreported. They typically present as soft, rubbery, dome-shaped lumps that are easily movable under the skin when pressed — a characteristic described as a doughy or fluctuant consistency.
Most lipomas are small, measuring between one and five centimeters in diameter, though they can occasionally grow much larger, with giant lipomas exceeding ten centimeters reported in the literature. Lipomas develop most commonly on the trunk, upper extremities, upper thighs, and shoulders, but can occur virtually anywhere on the body where fat tissue exists. They are typically painless and are discovered incidentally when the person notices a new lump during bathing or dressing.
Lipomas usually appear in adults between the ages of 40 and 60, though they can develop at any age including childhood. Men and women are affected approximately equally, with some studies suggesting a slight male predominance. Lipomas are almost always solitary, but approximately 5 to 15 percent of affected individuals develop multiple lipomas, a condition known as lipomatosis. Despite their classification as tumors, lipomas are definitively benign — they grow slowly, do not invade surrounding tissues, and have essentially no risk of malignant transformation.
What Causes Lipomas?
The exact cause of lipomas is not completely understood, but research has identified several factors that contribute to their development. Genetic predisposition is a major factor — lipomas frequently run in families, and several hereditary conditions feature multiple lipomas as a prominent characteristic. Familial multiple lipomatosis is an autosomal dominant condition in which affected individuals develop dozens to hundreds of lipomas throughout their lifetime.
Dercum's disease (adiposis dolorosa) is a condition characterized by multiple painful lipomas, primarily affecting postmenopausal women. Madelung's disease (multiple symmetric lipomatosis) causes symmetric fat deposits around the neck and shoulders and is associated with alcohol use and metabolic abnormalities. Bannayan-Riley-Ruvalcaba syndrome involves lipomas, macrocephaly, and intestinal polyps and is linked to mutations in the PTEN tumor suppressor gene.
At the cellular level, lipomas often harbor chromosomal rearrangements, particularly involving chromosome 12q13-15 and the HMGA2 gene, a transcription factor involved in cell growth and differentiation. These are somatic mutations occurring in individual fat cells rather than inherited mutations, and they are believed to trigger the localized proliferation of adipocytes that forms the lipoma. Trauma has been proposed as a trigger for lipoma development in some cases — the posttraumatic lipoma theory suggests that blunt injury to subcutaneous tissue may stimulate adipocyte proliferation or release pre-existing fat lobules from fascial constraints.
However, this association remains debated. Obesity does not cause lipomas — they occur with similar frequency in thin and obese individuals — though the lipomas may be more difficult to detect clinically in patients with abundant subcutaneous fat.
How to Identify a Lipoma
Lipomas have several characteristic clinical features that often allow confident diagnosis based on physical examination alone. The hallmark feature is a soft, rubbery, compressible mass that is freely mobile beneath the skin.!! When you press on a lipoma, it feels doughy and can be moved around with gentle finger pressure — it slips and slides under the skin because it is encapsulated and not attached to surrounding structures.
This mobility distinguishes lipomas from many other subcutaneous masses. The overlying skin appears completely normal — there is no discoloration, dimpling, or skin changes unless the lipoma is very superficial or has been traumatized. Most lipomas are round or oval, symmetric, and have smooth, well-defined margins that you can trace with your fingers.
They grow slowly over months to years and are typically painless, though a subtype called angiolipoma contains prominent blood vessels and can be tender to the touch, particularly in the forearms of young adults. On imaging, lipomas have a characteristic appearance that aids diagnosis when clinical examination is inconclusive. Ultrasound shows a well-circumscribed, elliptical, homogeneously hyperechoic (bright) mass in the subcutaneous tissue.
MRI is the gold standard imaging modality, revealing a well-encapsulated mass that precisely follows fat signal intensity on all sequences — bright on T1-weighted images and intermediate on T2-weighted images with suppression on fat-saturated sequences. These imaging characteristics are highly specific for lipoma and help distinguish it from more concerning soft tissue masses.
Lipoma vs. Liposarcoma: When a Fatty Lump Is Dangerous
The primary diagnostic concern with any new subcutaneous mass is distinguishing a benign lipoma from a liposarcoma — a malignant tumor of fat cells. While liposarcomas are rare (accounting for approximately 15 to 20 percent of soft tissue sarcomas, with an incidence of roughly one per 100,000 per year), they can initially resemble lipomas and the consequences of missing a liposarcoma are serious. Several features help distinguish between the two.
Size is an important factor — lipomas are usually under five centimeters, while liposarcomas tend to be larger at presentation, often exceeding five centimeters. Rapid growth is atypical for lipomas, which enlarge slowly over years; a mass that grows noticeably over weeks to months should raise suspicion. Location matters: lipomas are most common in the subcutaneous tissue, while liposarcomas more commonly develop in the deep soft tissues of the thigh, retroperitoneum, and trunk.
Consistency can provide clues — lipomas are uniformly soft and compressible, while liposarcomas may be firmer, harder, or contain areas of variable consistency. Lipomas are freely mobile; liposarcomas may be fixed to deeper structures. Pain is uncommon in lipomas (except angiolipomas); deep-seated or persistent pain in a fatty mass warrants evaluation.
On MRI, liposarcomas typically show heterogeneity — areas of non-fatty tissue, thick septa, nodular enhancement with contrast — rather than the homogeneous fat signal of a benign lipoma. The critical clinical rule is this: any subcutaneous mass that is larger than five centimeters, deep to fascia, growing rapidly, firm or hard, fixed, or painful should be imaged and potentially biopsied to rule out sarcoma, regardless of how much it resembles a typical lipoma.!!
Treatment: When and How to Remove Lipomas
Because lipomas are benign, treatment is not mandatory. Many patients with small, asymptomatic lipomas choose observation with periodic clinical monitoring. However, removal may be indicated or desired for several reasons: cosmetic concerns, particularly for lipomas in visible locations like the neck, arms, or forehead; pain or discomfort, especially with angiolipomas or lipomas pressing on nerves; functional impairment if the lipoma restricts movement or compresses adjacent structures; progressive growth that raises concern or causes physical problems; diagnostic uncertainty where biopsy is needed to confirm the diagnosis and exclude liposarcoma; or patient preference for definitive removal rather than ongoing monitoring.
Surgical excision is the standard treatment and provides definitive cure with very low recurrence rates (approximately one to two percent). The procedure involves making an incision over the lipoma, carefully dissecting the encapsulated mass from surrounding tissues, and removing it intact. Most subcutaneous lipomas can be removed under local anesthesia as an outpatient procedure.
The excised tissue is sent for histopathological examination to confirm the diagnosis. Liposuction can be used for larger lipomas, inserting a cannula through a small incision to aspirate the fatty tissue. While this approach leaves a smaller scar, it does not remove the capsule and has a higher recurrence rate.
It also does not provide intact tissue for pathological analysis, which is a significant limitation if there is any diagnostic uncertainty. Minimal excision (squeeze technique) combines a small incision with manual expression of the lipoma, offering smaller scars than traditional excision. Steroid injections (triamcinolone acetonide injected directly into the lipoma) can reduce lipoma size but rarely eliminate them completely. This approach may be considered for patients who want to avoid surgery.

How AI Skin Analysis Can Help
Discovering a new lump under your skin inevitably raises questions and often anxiety. Is it a lipoma? Could it be something more serious?
Skinscanner provides initial AI-powered assessment when you photograph and describe a subcutaneous lump, evaluating visible characteristics such as the appearance of the overlying skin, the outline of the mass, and its location on the body. While subcutaneous lumps present a unique challenge for image-based analysis — much of the diagnostic information comes from palpation (how the lump feels) rather than visual appearance alone — Skinscanner can help identify surface features and distribution patterns that suggest a benign lipoma versus features warranting more thorough investigation. The app provides educational context about subcutaneous lumps, helping you understand what features to assess when you feel a new lump — mobility, consistency, size, pain, and growth rate — and which features should prompt professional evaluation.
For individuals with known lipomas, regular documentation through Skinscanner helps track size changes over time, providing objective evidence of stability (reassuring) or growth (potentially requiring re-evaluation). This visual monitoring record is also valuable information to share with your physician during consultations. Skinscanner does not replace clinical examination for subcutaneous masses — proper evaluation of lumps under the skin requires physical palpation, and concerning masses need imaging (ultrasound or MRI) and potentially biopsy. But as a first-line information tool, Skinscanner helps you understand your finding and make an informed decision about when to seek professional evaluation.
