

เดอร์มาโทไฟโบรมา คืออะไร?
เดอร์มาโทไฟโบรมา — หรือที่รู้จักกันในชื่อฮิสติโอไซโตมาที่ไม่เป็นอันตรายหรือฮิสติโอไซโตมาที่ผิวหนัง — เป็นการเจริญเติบโตของผิวหนังที่ไม่เป็นอันตรายและพบได้ทั่วไป ซึ่งประกอบด้วยการผสมผสานของไฟโบรบลาสต์ คอลลาเจน และฮิสติโอไซต์ที่ก่อตัวเป็นก้อนกลมแข็งภายในชั้นหนังแท้ ก้อนเหล่านี้เป็นหนึ่งในอาการผิวหนังที่พบบ่อยที่สุดในทางการแพทย์ด้านผิวหนัง คิดเป็นประมาณสามเปอร์เซ็นต์ของตัวอย่างผิวหนังทั้งหมดที่ส่งไปยังการวิเคราะห์ทางพยาธิวิทยา เดอร์มาโทไฟโบรมามักปรากฏเป็นก้อนกลมถึงรูปไข่ที่แข็งซึ่งมีขนาดเส้นผ่านศูนย์กลางระหว่างห้าถึงสิบมิลลิเมตร แม้ว่าบางครั้งอาจมีขนาดถึงสองเซนติเมตรหรือใหญ่กว่า พวกมันรู้สึกเหมือนปุ่มแข็งขนาดเล็กที่ฝังอยู่ในผิวหนัง — แข็งกว่าผิวหนังรอบข้างอย่างชัดเจน ผิวหนังที่ปกคลุมอาจมีสีผิว สีชมพู สีน้ำตาลแดง หรือมีสีเข้มเกินไป และพื้นผิวมักจะเรียบ แต่บางครั้งอาจมีลักษณะเป็นขุยหรือเงา เดอร์มาโทไฟโบรมามักเกิดขึ้นที่ส่วนล่างของร่างกาย โดยเฉพาะที่น่องและต้นขา แม้ว่าจะสามารถพัฒนาได้ทุกที่บนร่างกาย พวกมันพบได้บ่อยในผู้หญิงมากกว่าผู้ชาย โดยส่วนใหญ่จะปรากฏในผู้ใหญ่ที่อายุน้อยถึงกลางคนระหว่างอายุ 20 ถึง 50 ปี ก้อนเหล่านี้มักจะเกิดขึ้นเพียงก้อนเดียว — การมีมากกว่าหนึ่งก้อนนั้นเป็นเรื่องปกติ แต่เดอร์มาโทไฟโบรมาหลายก้อนพร้อมกันอาจเกี่ยวข้องกับการมีภูมิคุ้มกันต่ำ เมื่อก่อตัวแล้ว เดอร์มาโทไฟโบรมามักจะถาวรและมีเสถียรภาพ ไม่เติบโตอย่างมีนัยสำคัญหรือหายไปเอง

สาเหตุของเดอร์มาโทไฟโบรมา คืออะไร?
สาเหตุที่แน่ชัดของเดอร์มาโทไฟโบรมายังไม่ได้รับการยืนยันอย่างเต็มที่ แต่เชื่อกันอย่างกว้างขวางว่ามันเป็นการเจริญเติบโตของเนื้อเยื่อเส้นใยที่เกิดจากการตอบสนองต่อการบาดเจ็บเล็กน้อยที่ผิวหนัง ผู้ป่วยหลายคนสามารถจำได้ถึงการถูกแมลงกัด การถูกหนามทิ่ม การมีเศษไม้เข้าไป การบาดเจ็บเล็กน้อย หรือการอักเสบของรูขุมขนที่บริเวณที่เดอร์มาโทไฟโบรมาเกิดขึ้น ซึ่งสนับสนุนทฤษฎีการเกิดจากการตอบสนองต่อการบาดเจ็บ ความคิดคือการบาดเจ็บเล็กน้อยหรือการถูกแมลงกัดจะกระตุ้นการตอบสนองการอักเสบในบริเวณที่เกิดขึ้น และในระหว่างกระบวนการรักษา ไฟโบรบลาสต์และเซลล์อื่น ๆ จะเจริญเติบโตมากเกินไป สร้างก้อนเนื้อเยื่อเส้นใยที่หนาแน่นซึ่งยังคงอยู่หลังจากที่กระตุ้นเริ่มต้นได้หายไป อย่างไรก็ตาม เดอร์มาโทไฟโบรมาหลายก้อนปรากฏขึ้นโดยไม่มีการบาดเจ็บที่สามารถระบุได้ ซึ่งบ่งชี้ว่ามีปัจจัยอื่น ๆ ที่มีส่วนเกี่ยวข้อง อิทธิพลทางฮอร์โมนอาจมีส่วนร่วม — การมีอัตราการเกิดสูงขึ้นในผู้หญิงและการปรากฏหรือขยายตัวในระหว่างการตั้งครรภ์สนับสนุนสมมติฐานนี้ ระบบภูมิคุ้มกันก็มีบทบาทเช่นกัน เนื่องจากบุคคลที่มีภูมิคุ้มกันต่ำจากการติดเชื้อ HIV การปลูกถ่ายอวัยวะ หรือการใช้ยากดภูมิคุ้มกันมีแนวโน้มที่จะพัฒนาเดอร์มาโทไฟโบรมาได้มากกว่า โดยมีแนวโน้มที่จะเกิดขึ้นในหลายก้อน ความโน้มเอียงทางพันธุกรรมอาจมีอยู่ เนื่องจากบางคนพัฒนาเดอร์มาโทไฟโบรมาได้มากมายในขณะที่คนอื่นไม่เคยพัฒนาเลยแม้จะมีการสัมผัสกับการบาดเจ็บที่ผิวหนังเล็กน้อยก็ตาม ในระดับเซลล์ เดอร์มาโทไฟโบรมาประกอบด้วยการผสมผสานของไฟโบรบลาสต์ ไมโอไฟโบรบลาสต์ ฮิสติโอไซต์ และเซลล์อักเสบที่จัดเรียงในรูปแบบที่เป็นเอกลักษณ์ในชั้นหนังแท้ เลสชันมักจะขยายไปถึงไขมันใต้ผิวหนังและจับกลุ่มคอลลาเจนที่อยู่รอบ ๆ ที่ขอบ ทำให้เกิดความแข็งที่เป็นเอกลักษณ์ของก้อนเหล่านี้

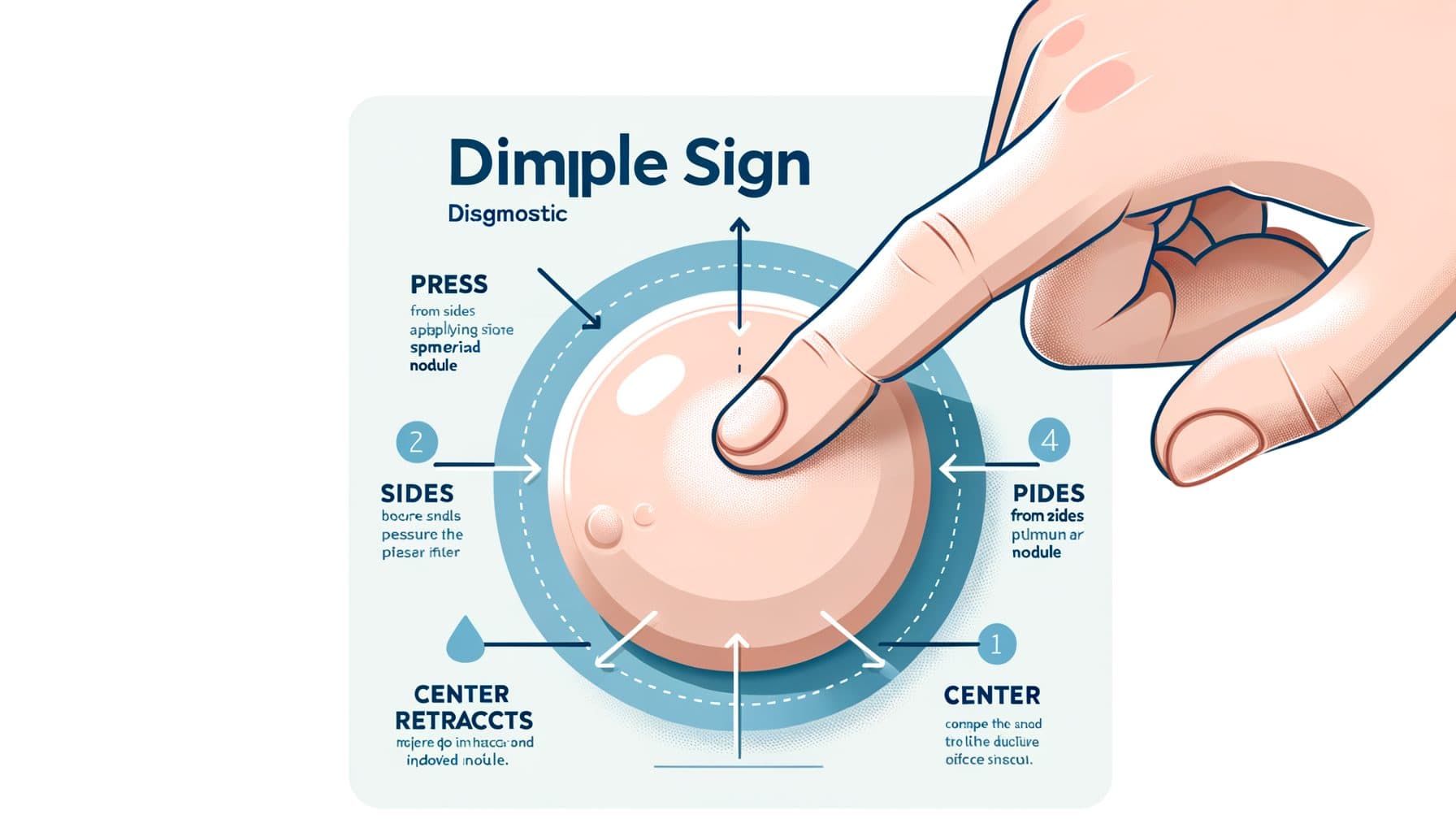
สัญญาณบุ๋ม: เบาะแสการวินิจฉัย
เมื่อคุณบีบผิวหนังที่อยู่เหนือ dermatofibroma ระหว่างนิ้วโป้งและนิ้วชี้ เลสชันจะมีลักษณะยุบตัวหรือดึงเข้าด้านในแทนที่จะยื่นออกไปข้างนอกเหมือนเลสชันผิวหนังที่ยกสูงส่วนใหญ่!! สิ่งนี้เกิดขึ้นเนื่องจาก dermatofibromas ถูกยึดติดกับผิวหนังรอบข้างโดยการขยายตัวที่มีลักษณะคล้ายหนวด และการบีบด้านข้างทำให้เลสชันถูกดึงลงไปในเนื้อเยื่อใต้ผิวหนัง สัญญาณ dimple มีลักษณะเฉพาะมากจนสามารถสร้างการวินิจฉัยทางคลินิกได้เพียงอย่างเดียวในกรณีส่วนใหญ่ แม้ว่าจะไม่เฉพาะเจาะจงทั้งหมด — เลสชันมะเร็งที่หายากสามารถสร้างสัญญาณที่คล้ายกันได้ ในการระบุ dermatofibromas ยังมีลักษณะอื่น ๆ ที่ช่วยได้ พวกมันมีความแข็งแรงอย่างน่าทึ่งเมื่อสัมผัส — แข็งกว่าผิวหนังรอบข้างและเลสชันผิวหนังที่ไม่เป็นอันตรายอื่น ๆ ส่วนใหญ่ ผิวหนังที่อยู่เหนือมักจะแสดงการเปลี่ยนสีเป็นสีน้ำตาลซึ่งอาจเข้มขึ้นเมื่อสัมผัสกับแสงแดด ในการตรวจด้วย dermoscopy, dermatofibromas แสดงรูปแบบที่มีลักษณะเฉพาะ: พื้นที่สีขาวกลางที่คล้ายแผลเป็นล้อมรอบด้วยเครือข่ายสีผิวที่ละเอียดอ่อน บางครั้งถูกอธิบายว่าดูเหมือนแผ่นสีขาวที่ล้อมรอบด้วยวงแหวนสีน้ำตาลที่มีลักษณะคล้ายลูกไม้ รูปแบบนี้แตกต่างจากเครือข่ายสีผิวที่เห็นในเลสชัน melanocytic และสามารถรับรู้ได้โดยแพทย์ที่ได้รับการฝึกอบรม การยึดติดของ dermatofibromas ภายในผิวหนังเป็นลักษณะเฉพาะอีกอย่างหนึ่ง — พวกมันเคลื่อนที่ไปกับผิวหนังเมื่อคุณเลื่อนมันไปบนเนื้อเยื่อที่อยู่ใต้ แต่รู้สึกเหมือนถูกยึดติดอยู่ภายในผิวหนังเอง แตกต่างจาก lipomas ที่เคลื่อนไหวได้อย่างอิสระใต้ผิวหนัง.
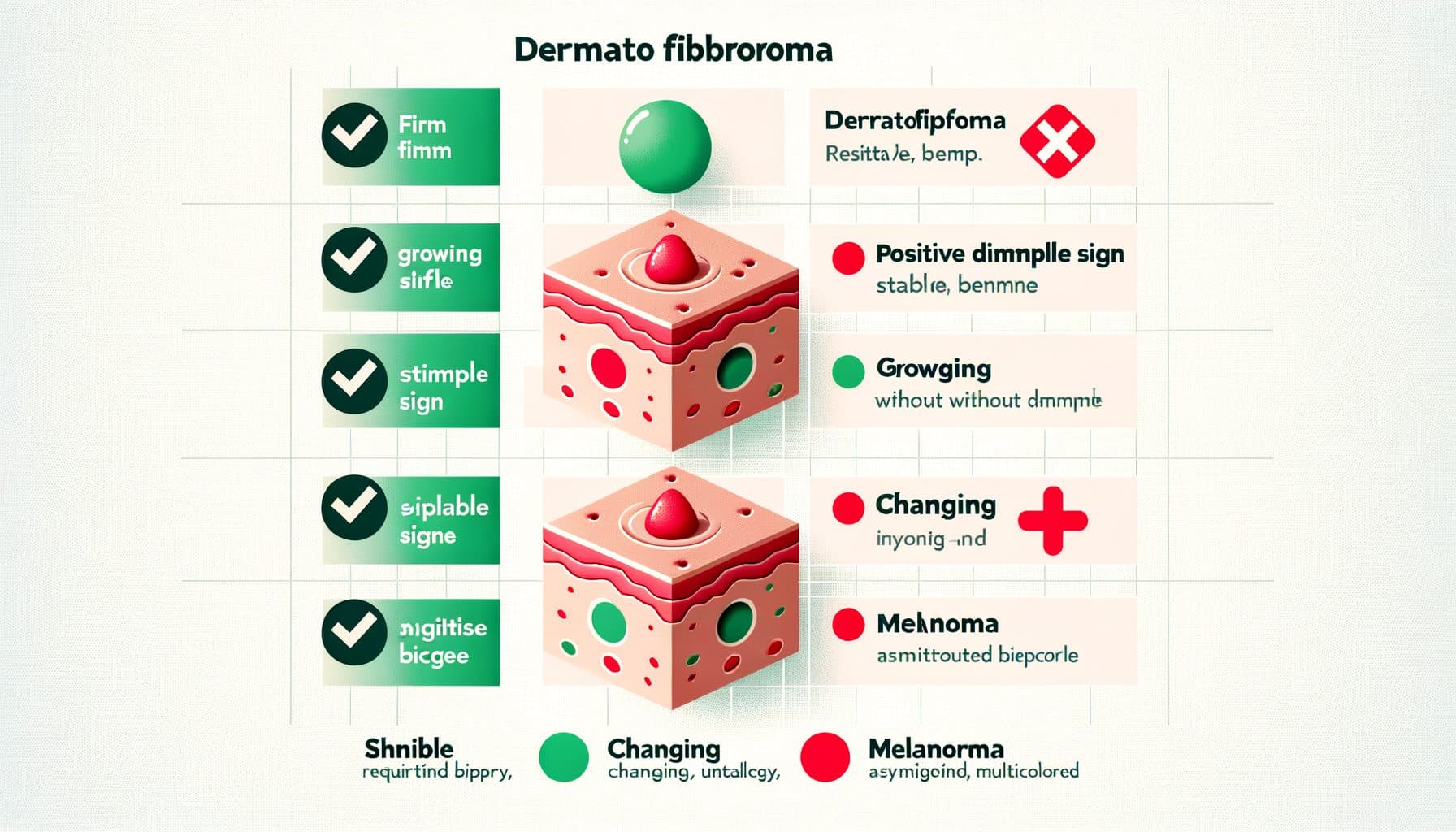
Dermatofibroma vs. เลสชันที่น่ากังวลมากขึ้น
ก้อนเนื้อใด ๆ ที่เติบโตเกินสองเซนติเมตร ขยายตัวอย่างต่อเนื่อง หรือยึดติดกับโครงสร้างที่ลึกกว่าควรได้รับการตรวจชิ้นเนื้อเพื่อแยกแยะ DFSP!! เมลาโนมาอาจปรากฏเป็นก้อนเนื้อที่แข็งและมีสีที่อาจถูกสับสนกับ dermatofibroma ที่มีสีเข้ม ลักษณะที่บ่งบอกถึงเมลาโนมารวมถึงความไม่สมมาตร ขอบที่ไม่สม่ำเสมอ การเปลี่ยนแปลงสีรวมถึงเฉดสีฟ้า-ดำหรือแดง และการเปลี่ยนแปลงขนาดหรืออาการในช่วงเวลาล่าสุด สัญญาณ dimple มักจะไม่มีในเมลาโนมา มะเร็งเซลล์ฐาน โดยเฉพาะอย่างยิ่งประเภท morpheaform หรือ nodular อาจปรากฏเป็นก้อนเนื้อที่แข็งและมีสีผิว มองหาคุณภาพที่โปร่งแสงเหมือนไข่มุก เส้นเลือดขอดบนพื้นผิว และการไม่มีสัญญาณ dimple มะเร็งเซลล์เมอเคิลอาจปรากฏเป็นก้อนเนื้อที่แข็ง เติบโตอย่างรวดเร็ว มีสีแดงถึงม่วง มักจะอยู่บนผิวหนังที่สัมผัสกับแสงแดดในผู้สูงอายุ ก้อนเนื้อใด ๆ ที่กำลังเติบโต เปลี่ยนแปลง ลักษณะอาการเจ็บปวด เลือดออก หรือมีแผลควรได้รับการตรวจชิ้นเนื้อไม่ว่าจะมีลักษณะคล้ายกับ dermatofibroma แบบทั่วไปเพียงใด บริบทมีความสำคัญ — ก้อนเนื้อที่แข็งในผู้ป่วยที่มีภูมิคุ้มกันต่ำหรือผู้ที่มีประวัติมะเร็งผิวหนังควรได้รับการตรวจชิ้นเนื้อในเกณฑ์ที่ต่ำกว่า.
การรักษา: เมื่อใดและอย่างไรในการกำจัด dermatofibromas
เนื่องจาก dermatofibromas เป็นก้อนเนื้อที่ไม่เป็นอันตรายและไม่มีความเสี่ยงต่อการเปลี่ยนแปลงเป็นมะเร็ง การรักษาจึงไม่จำเป็นทางการแพทย์ ผู้ป่วยหลายคนเรียนรู้ที่จะอยู่กับ dermatofibromas ของพวกเขาหลังจากที่เข้าใจธรรมชาติที่ไม่เป็นอันตรายของการเจริญเติบโต อย่างไรก็ตาม การกำจัดอาจเป็นที่ต้องการด้วยเหตุผลหลายประการ: ความกังวลด้านความงาม โดยเฉพาะอย่างยิ่งสำหรับเลสชันที่อยู่ในพื้นที่ที่มองเห็นได้เช่นหน้าแข้งหรือแขน; การระคายเคืองซ้ำจากการโกน การเสียดสีจากเสื้อผ้า หรือการบาดเจ็บซ้ำ; ความเจ็บปวดหรือความไวที่คงอยู่ (บาง dermatofibromas อาจไม่สบายเมื่อถูกกด); ความไม่แน่นอนในการวินิจฉัยซึ่งต้องการการตรวจชิ้นเนื้อเพื่อแยกแยะเลสชันที่น่ากังวลมากขึ้น; หรือความวิตกกังวลของผู้ป่วยที่สำคัญแม้จะได้รับการยืนยันแล้ว การตัดออกทั้งหมดเป็นการรักษาที่แน่นอน แต่มีข้อควรระวังที่สำคัญ: เนื่องจาก dermatofibromas ขยายลึกเข้าไปในผิวหนังและบางครั้งเข้าไปในไขมันใต้ผิวหนัง การตัดออกทั้งหมดจะต้องตัดลึกพอสมควร ส่งผลให้เกิดแผลเป็นจากการผ่าตัดที่อาจเห็นได้ชัดเจนมากกว่าเลสชันเดิม — โดยเฉพาะอย่างยิ่งที่ขาซึ่งการรักษาแผลเป็นมักจะช้ากว่าและเห็นได้ชัดเจนมากขึ้น ผู้ป่วยควรได้รับคำปรึกษาเกี่ยวกับการแลกเปลี่ยนนี้ก่อนที่จะดำเนินการ การตัดเฉือนแบบโกน (การกำจัดแบบขนาน) จะกำจัดส่วนที่มองเห็นของ dermatofibroma ที่อยู่ระดับเดียวกับหรืออยู่ใต้ผิวหนัง ทำให้แผลเป็นเรียบกว่า อย่างไรก็ตาม เนื่องจากส่วนที่ลึกกว่ายังคงอยู่ อัตราการกลับเป็นซ้ำจะสูงขึ้น — รายงานที่ 20 เปอร์เซ็นต์หรือมากกว่า การรักษาด้วยความเย็นด้วยไนโตรเจนเหลวสามารถทำให้ dermatofibromas แบนลง แต่แทบจะไม่สามารถกำจัดพวกมันได้ทั้งหมดและอาจทิ้งรอยด่างขาว การรักษาด้วยเลเซอร์ได้ถูกนำมาใช้ด้วยความสำเร็จที่แตกต่างกัน สำหรับผู้ป่วยส่วนใหญ่ วิธีการที่เหมาะสมคือการสังเกตพร้อมกับการยืนยัน โดยการตัดออกจะสงวนไว้สำหรับเลสชันที่มีอาการ ไม่แน่นอนในการวินิจฉัย หรือก่อให้เกิดความเครียดด้านความงามที่สำคัญ.

AI Skin Analysis สามารถช่วยได้อย่างไร
การค้นพบก้อนเนื้อที่แข็งในผิวหนังของคุณทำให้เกิดคำถามและบางครั้งความวิตกกังวล เป็นเพียง dermatofibroma ที่ไม่เป็นอันตรายหรืออาจเป็นสิ่งที่ร้ายแรงกว่านั้น? Skinscanner ให้การวิเคราะห์ที่ขับเคลื่อนด้วย AI ทันทีเมื่อคุณถ่ายภาพก้อนเนื้อผิวหนังที่น่ากังวล โดยประเมินลักษณะต่าง ๆ เช่น สี รูปร่าง ลักษณะขอบ และพื้นผิวเพื่อช่วยในการกำหนดว่าเลสชันนั้นสอดคล้องกับ dermatofibroma ที่ไม่เป็นอันตรายหรือมีลักษณะที่ต้องการการประเมินจากผู้เชี่ยวชาญ AI สามารถรับรู้รูปแบบทั่วไปที่เกี่ยวข้องกับ dermatofibromas — การเปลี่ยนสีเป็นสีน้ำตาล รูปร่างกลมสมมาตร และพื้นผิวเรียบ — และแยกแยะพวกมันออกจากรูปแบบที่บ่งบอกถึงเลสชันที่น่ากังวลมากขึ้น เช่น dermatofibrosarcoma protuberans หรือเมลาโนมา สำหรับบุคคลที่มี dermatofibromas หลายตัว Skinscanner ช่วยติดตามเลสชันที่มีอยู่สำหรับการเปลี่ยนแปลงใด ๆ และระบุการเจริญเติบโตใหม่ที่แตกต่างจากรูปแบบที่มีอยู่ ในขณะที่สัญญาณ dimple ที่เป็นเอกลักษณ์ไม่สามารถประเมินได้จากการถ่ายภาพเพียงอย่างเดียว แต่ลักษณะภาพที่บันทึกไว้ในภาพถ่ายคุณภาพสูงให้ข้อมูลวินิจฉัยที่มีค่า Skinscanner มีประโยชน์โดยเฉพาะอย่างยิ่งในฐานะเครื่องมือคัดกรองเบื้องต้นสำหรับสถานการณ์ทั่วไปในการค้นพบก้อนเนื้อใหม่ที่แข็งและต้องการคำแนะนำทันทีว่าจำเป็นต้องมีการประเมินอย่างเร่งด่วนหรือไม่ มันไม่สามารถแทนที่การตรวจสอบทางคลินิกได้ — ก้อนเนื้อใด ๆ ที่กำลังเติบโต เปลี่ยนแปลง มีอาการ หรือก่อให้เกิดความกังวลแม้จะได้รับการยืนยันจาก AI ควรได้รับการประเมินโดยแพทย์ผิวหนังที่สามารถทำการตรวจสอบ การตรวจด้วย dermoscopy และการตรวจชิ้นเนื้อหากจำเป็น.
