

What Is Onychomycosis and Why Is It So Common?
Onychomycosis — the medical term for fungal nail infection — is caused by dermatophyte fungi (most commonly Trichophyton rubrum and Trichophyton mentagrophytes), yeasts (particularly Candida species), and non-dermatophyte molds. Dermatophytes account for approximately 90% of toenail infections and a smaller proportion of fingernail infections. The condition affects roughly 14% of the general population in North America and Europe, with prevalence increasing sharply with age — nearly half of people over 70 have at least one affected nail.
Toenails are affected far more often than fingernails (approximately 80% of cases) because feet spend more time in warm, moist environments (shoes and socks) that favor fungal growth, have reduced blood circulation compared to hands (impeding immune defense), and are more likely to encounter fungi on contaminated surfaces. Risk factors include advancing age (slower nail growth, reduced circulation, decades of fungal exposure), diabetes (impaired immunity and circulation), peripheral vascular disease, immunosuppression, athlete's foot (tinea pedis, which often serves as the source of nail infection), nail trauma or damage, working in wet environments, and use of communal showers or pools. Genetic susceptibility also plays a role — some families have a markedly higher prevalence, suggesting inherited variations in immune response to dermatophytes.
Onychomycosis is far more than a cosmetic concern: affected nails can become thick and difficult to trim, cause pain when wearing shoes, create entry points for bacterial infections (particularly dangerous for diabetics), and significantly impact quality of life and psychological wellbeing. In diabetic patients, onychomycosis increases the risk of foot ulcers and secondary infections that can ultimately lead to amputation.

Types of Nail Fungus: Patterns of Infection
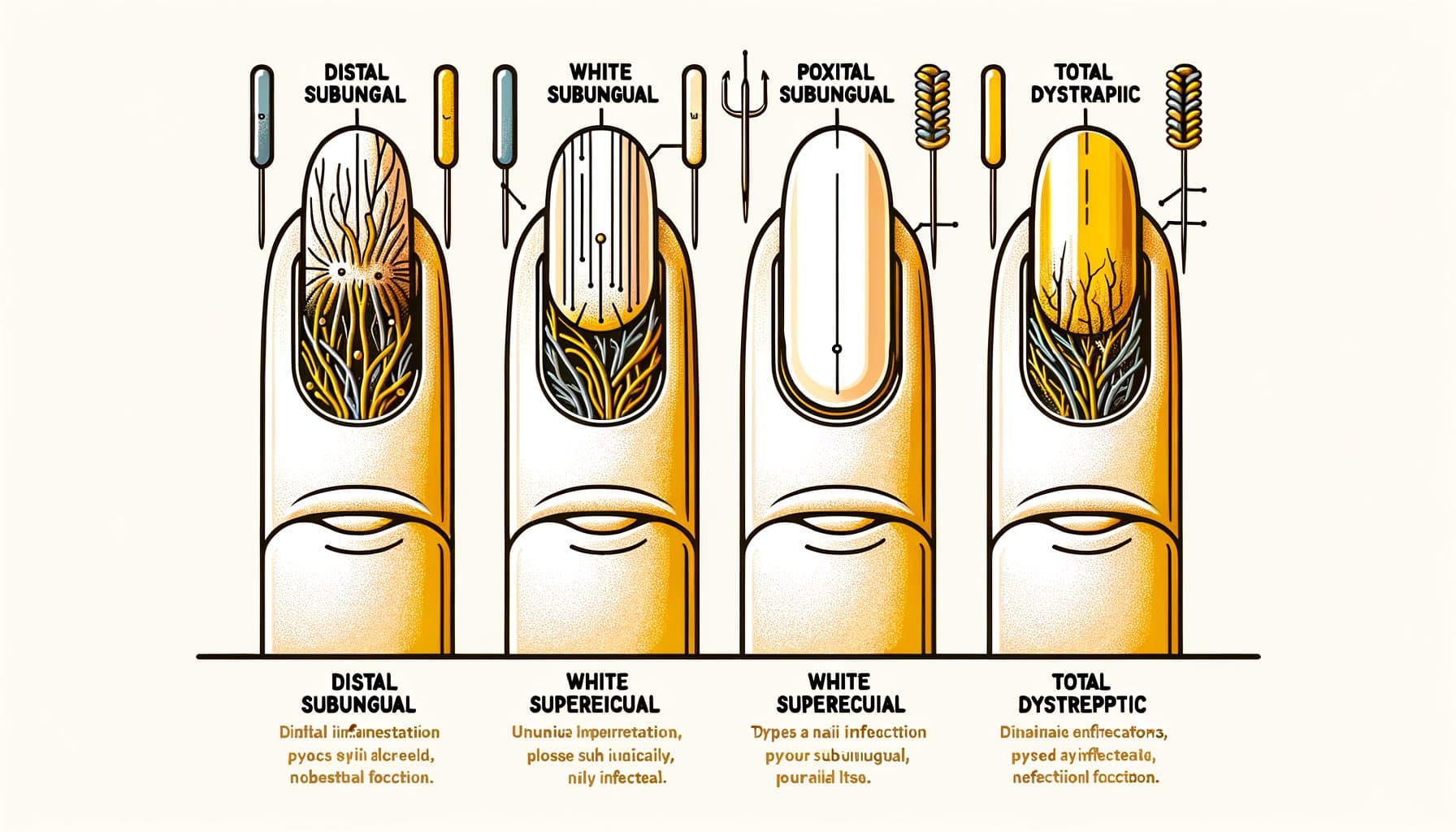
Onychomycosis presents in several distinct clinical patterns, each reflecting a different route of fungal invasion. Distal lateral subungual onychomycosis (DLSO) is the most common type, accounting for approximately 75% of cases. The fungus invades under the free edge of the nail (the tip you trim) and the lateral nail folds, then spreads toward the cuticle.
The hallmarks are yellowing or brownish discoloration beginning at the nail tip and progressing toward the base, subungual debris (crumbly material accumulating under the nail), and gradual nail thickening. Proximal subungual onychomycosis (PSO) is relatively uncommon in healthy individuals but is the most common pattern in immunocompromised patients, particularly those with HIV. The fungus enters through the proximal nail fold (near the cuticle) and spreads toward the nail tip — the opposite direction of DLSO.
A white or opaque area appearing near the cuticle in an otherwise healthy-looking nail, particularly in a younger person, should raise suspicion for immune compromise. White superficial onychomycosis (WSO) presents as white, chalky, friable patches on the nail surface. Unlike other types where the fungus invades deep within or under the nail, WSO involves fungal colonization of the outer nail plate surface.
This makes it the easiest type to treat — topical antifungals can directly reach the infection. Total dystrophic onychomycosis (TDO) represents end-stage disease where the entire nail is thickened, crumbling, and destroyed by fungal infection. TDO can develop as the progression of any of the above subtypes left untreated over months to years.
Candidial onychomycosis is primarily caused by Candida species and more commonly affects fingernails, particularly in individuals with chronic moisture exposure (dishwashers, bartenders, laundry workers). It often involves the proximal and lateral nail folds with associated swelling and tenderness (paronychia). Accurate identification of the pattern helps guide treatment decisions and can provide clues about underlying health status.
Diagnosis: Why Confirmation Matters Before Treatment
An important principle in onychomycosis management is confirming the diagnosis before committing to treatment — especially oral antifungal treatment. Up to 50% of dystrophic (abnormal-appearing) nails are not actually caused by fungal infection.!! Conditions that mimic onychomycosis include nail psoriasis (one of the most common mimics, causing pitting, discoloration, and thickening), nail trauma (repeated microtrauma from tight shoes or running), lichen planus of the nail, melanonychia (dark nail discoloration from melanin), and nail changes from dermatitis or poor circulation.
Treating a non-fungal nail condition with months of antifungal medication is ineffective, expensive, and exposes you to unnecessary drug side effects. Diagnostic methods include potassium hydroxide (KOH) preparation, where nail scrapings are dissolved in KOH solution and examined under a microscope for fungal elements — results available within minutes, sensitivity approximately 70-80%. Fungal culture involves sending nail clippings or scrapings to a laboratory to identify the specific organism — results take 3-6 weeks but provide species identification that can guide treatment choice.
PAS (periodic acid-Schiff) staining of nail clippings examined histologically has the highest sensitivity (over 90%) and takes 1-2 days. PCR-based molecular testing is newer, faster, and highly sensitive but not universally available. A negative KOH or culture does not definitively rule out onychomycosis (false negatives are common), so repeat testing or alternative methods may be needed if clinical suspicion remains high. Conversely, a positive laboratory result combined with compatible clinical appearance provides the confidence to embark on a prolonged treatment course knowing the diagnosis is correct.

Treatment: Oral vs. Topical and Realistic Expectations
Treatment of onychomycosis requires patience and realistic expectations — even with the most effective treatments, complete cure rates are far from 100%, and visible improvement is slow because healthy nail must grow out to replace the damaged nail. Toenails grow at approximately 1-2mm per month, meaning complete toenail replacement takes 12-18 months. Fingernails grow faster (3-4mm/month) with full replacement in 6-9 months.
Oral antifungal medications are the most effective treatment for moderate to severe onychomycosis. Terbinafine (Lamisil) is the gold standard for dermatophyte infections, taken daily for 6 weeks (fingernails) or 12 weeks (toenails), with mycological cure rates of 70-80% and complete cure rates of 38-50%. It is generally well-tolerated but requires baseline and periodic liver function monitoring, as rare cases of hepatotoxicity occur.
Common side effects include gastrointestinal upset, taste disturbance, and headache. Itraconazole (Sporanox) is an alternative, often used in pulse dosing (one week on, three weeks off, repeated for 2-3 cycles), effective against a broader range of fungi including Candida. It has more drug interactions than terbinafine and requires liver monitoring.
Fluconazole is sometimes used off-label in weekly dosing for prolonged periods. Topical treatments are less effective than oral medications for most types of onychomycosis because the nail plate acts as a barrier preventing drug penetration to the nail bed and matrix where the infection resides. Ciclopirox nail lacquer (Penlac) was the first FDA-approved topical, with modest cure rates of approximately 5-10%.
Efinaconazole (Jublia) and tavaborole (Kerydin) are newer topical solutions with improved penetration and cure rates of approximately 15-20%. Topical treatments are most appropriate for mild, early infections, white superficial onychomycosis, patients who cannot take oral antifungals due to drug interactions or liver concerns, and as adjuncts to oral therapy to improve cure rates. Combination therapy (oral plus topical) achieves higher cure rates than either alone.
Mechanical debridement — having thick, dystrophic nail professionally trimmed and thinned — improves both topical drug penetration and cosmetic appearance during the lengthy treatment process. Laser treatment has been marketed aggressively but evidence for efficacy remains limited and inconsistent, with most well-designed studies showing modest or no benefit over placebo.

Prevention: Keeping Fungus from Coming Back
Recurrence rates after successful onychomycosis treatment are high — estimated at 10-50% over several years — making prevention an essential long-term strategy. The most important preventive measures target the environmental conditions that fungi exploit. Keep feet dry: change socks daily (more often if feet sweat heavily), choose moisture-wicking synthetic or wool socks over cotton, alternate shoes daily to allow them to dry completely between wearings, and use antifungal powder or spray in shoes.
Treat athlete's foot promptly and completely, as tinea pedis is the most common source of nail fungal infection — the fungus spreads from infected skin between the toes to the nail bed. Protect feet in communal wet areas: wear sandals or water shoes in gym showers, locker rooms, pool decks, and hotel bathrooms. Maintain proper nail hygiene: trim nails straight across (don't round corners, which creates spaces for fungal entry), keep nails short, don't share nail clippers or files, and sterilize tools between uses with rubbing alcohol.
Avoid nail trauma: wear properly fitted shoes with adequate toe room, trim nails regularly to prevent them catching on socks, and protect toenails during sports and physical activity. Address underlying risk factors where possible: optimize blood sugar control in diabetes, discuss immunosuppressive medication adjustments with your physician, and improve peripheral circulation through regular exercise. Some dermatologists recommend prophylactic application of topical antifungal to previously infected nails after treatment completion — weekly application of antifungal nail lacquer or solution may prevent reinfection.
For individuals with chronic, recurrent onychomycosis, periodic courses of oral antifungal medication may be needed. Keeping nail tools sanitized, avoiding shared pedicure instruments at salons (bring your own or ensure proper sterilization), and treating all household members with fungal infections simultaneously prevents reinfection from shared surfaces.

When to See a Doctor About Nail Changes
Not every discolored or thick nail is fungal, and professional evaluation is important before starting treatment. See a healthcare provider if you notice progressive nail discoloration (yellowing, browning, or white patches), thickening that makes trimming difficult, crumbling or brittleness of the nail edge, separation of the nail from the nail bed, or pain in the affected nail. Diabetic patients should seek evaluation promptly for any nail changes, as onychomycosis increases their risk of secondary bacterial infection and foot ulcers.
If you have previously had nail fungus successfully treated and notice early signs of recurrence, early intervention is more effective than waiting for the infection to become established. A dark streak or band in the nail (melanonychia) requires urgent evaluation to rule out subungual melanoma — this is especially important if the streak is new, progressively widening, or associated with nail deformity or periungual pigmentation (Hutchinson sign).!! Pain, swelling, and redness around the nail fold (acute paronychia) may indicate bacterial infection requiring antibiotic treatment rather than antifungal therapy. If over-the-counter antifungal treatments have failed after 3-6 months of consistent use, professional diagnosis (to confirm the fungal etiology) and prescription treatment offer significantly higher cure rates.

How AI Skin Analysis Can Help Assess Nail Changes
Nail changes are common and have numerous potential causes — determining whether a discolored or thickened nail is due to fungal infection, psoriasis, trauma, or another condition is the essential first step before committing to months of treatment. Skinscanner provides an accessible preliminary assessment by analyzing photographs of your affected nails for features consistent with onychomycosis versus other nail conditions. By photographing your nails at the start of treatment and at monthly intervals, you create an objective record of treatment response that reveals slow, gradual improvement that might not be apparent in daily observation.
Given that toenail treatment takes 12-18 months to show full results, having a photographic timeline provides motivation to continue treatment and objective evidence to share with your healthcare provider when evaluating treatment efficacy. Skinscanner can also help you monitor for signs of recurrence after successful treatment — subtle early changes are easier to detect in comparative photographs than in casual inspection. While AI analysis cannot replace laboratory confirmation of fungal infection, it provides a valuable screening step that helps you decide whether professional evaluation is warranted and supports effective treatment monitoring once therapy begins.
